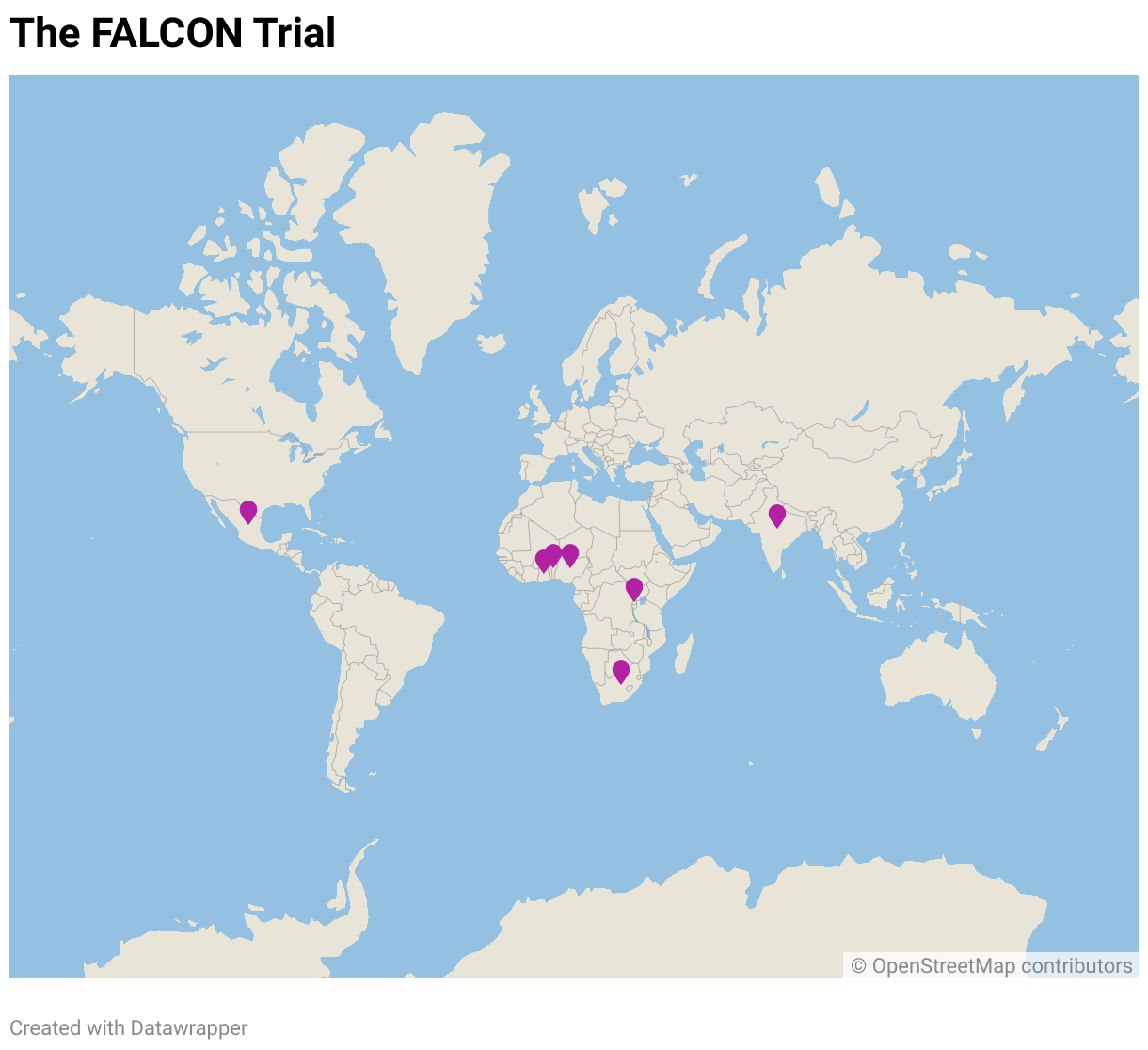
FALCON is the first global surgical trial testing measures to reduce Surgical Site Infection (SSI) following abdominal surgery in low and middle-income countries.
It was launched in December 2018 and on 07th September 2020, the final patients were randomised into the trial. In total, 5789 patients were randomised across three continents and seven countries – Mexico, Ghana, India, Nigeria, Rwanda, Benin and South Africa. With the recruitment phase having been projected to last approximately 3 years, FALCON was completed 15 months ahead of schedule – a great example of how collaboration can have truly inspiring results!
3
CONTINENTS
7
COUNTRIES
55
HOSPITALS
5800
PATIENTS RECRUITED
Background
Surgical site infection is the most common complication after surgery across the world. It is the commonest healthcare-associated infection in low and middle-income countries.
Surgical site infection (SSI) causes pain, discomfort, disability and prolongs the period before the patient can taken to return to work. As such, the surgical site infection costs to healthcare systems increase significantly creating burden on a personal and a society level. The increased costs can be a major problem in countries with lower income where patients often may require paying for their own treatment.
FALCON is an investigator-initiated and investigator-led trial funded by the UK National Institute for Health Research (NIHR).

Aims & Objectives
Primary Objective
The primary objective of main RCT is to assess whether either (1) 2% alcoholic chlorhexidine versus 10% povidone-iodine for skin preparation, or (2) triclosan-coated suture versus non-coated suture for fascial closure, can reduce surgical site infection at 30-days post-surgery for each of (i) clean-contaminated and (ii) contaminated or dirty abdominal surgery.
Secondary Objectives
- To assess the impact of the interventions on secondary clinical outcomes up to 30 days post-surgery including: SSI at discharge, mortality, unplanned wound opening, re-operation, length of hospital stay, re-admission, and return to normal activities.
- To assess the impact of the interventions on the resistance of organisms isolated from wound swabs to prophylactic antibiotics administered.
- To explore the impact of the interventions on service delivery and additional costs to the secondary health service provider.
- The recruitment target is 5788 participants across all centres.
Surgical site infection (SSI) represents a major burden for patients, doctors, and health systems across all settings. SSI is the commonest postoperative complication worldwide and the commonest healthcare-associated infection in low and middle income countries (LMICs). SSIs cause pain, discomfort, disability, and increase the time taken to return to work. SSIs increase health costs and this can have a major impact on patients, communities, and providers in LMICs where personal income is low and patients may be required to pay for their own treatment. SSI has also been associated with one-third of postoperative deaths and accounts for 8% of all deaths caused by a nosocomial infection.
The GlobalSurg-2 cohort study captured data on 12539 patients undergoing abdominal surgery across 343 hospitals in 66 countries, with a primary outcome measure of SSI. The overall SSI rate was 12.3% (1538/12539), which more than doubled across high, middle, and low human development index (HDI) countries (9.4%, 14.0%, 23.2%, respectively, p<0.001). The overall SSI rate in LMICs was 16.3% (847/5200). After risk adjustment for patient, disease, operative, and hospital factors, patients in low-income countries remained at greater risk of SSI than those in high-income countries (adjusted OR 1.60, 95% confidence interval 1.05-2.37, p=0.030). The overall SSI rates in children and adults were similar (12.1% vs. 12.3%).
Improving surgical outcomes is a global health priority, highlighted by the Lancet Commission on Global Surgery. Recent World Health Organisation (WHO) guidelines made 29 recommendations for intraoperative and postoperative measures to prevent SSI, including global perspectives relevant to LMICs. Despite inclusion of strongly graded recommendations, there was little high quality evidence in support of most interventions. In addition, none of the evidence used was derived from resource limited settings, leading to uncertainty about implementation of measures in these settings. A randomised trial with the potential to evaluate multiple interventions would establish a high quality evidence base that will inform guidance, and influence revisions to the WHO Surgical Safety Checklist. The specific interventions to be tested in the trial were selected by a Delphi process from a longlist of potential interventions based on the WHO guidelines.
The trial aims to assess whether either:
(1) 2% alcoholic chlorhexidine versus 10% povidone-iodine for skin preparation, or
(2) triclosan-coated suture versus non-coated suture for fascial closure, can reduce surgical site infection at 30-days post-surgery for each of:
(1) clean-contaminated or
(2) contaminated/dirty surgery.
FALCON is a pragmatic, patient and outcome assessor blinded, 2×2 factorial, stratified, multi-centre randomised controlled trial, with an internal pilot, to evaluate measures to reduce SSI rates in patients undergoing surgery with an abdominal incision. Strata are defined according to the anticipated category of wound contamination: (1) clean-contaminated and (2) contaminated/dirty.
Patients (adults and children) undergoing surgery with abdominal incision of at least ≥5cm, with an anticipated (1) clean-contaminated or (2) contaminated/dirty wound. Participants undergoing emergency or elective, and open or laparoscopic surgery are eligible.
Eligible patients will be randomised at the level of the individual in a 1:1:1:1 ratio between:
- 2% alcoholic chlorhexidine and non-coated suture
- 2% alcoholic chlorhexidine and triclosan-coated suture
- 10% aqueous povidone-iodine and non-coated suture
- 10% aqueous povidone-iodine and triclosan-coated suture

The FALCON trial has a 6-month internal pilot the aim of which is to assess:
- If recruitment to the randomised interventions is feasible
- Compliance with treatment allocation
- Patient retention and follow-up.
- Patients with at least one abdominal incision that is ≥5cm (open or laparoscopic extraction site), with an anticipated clean-contaminated, contaminated or dirty surgical wound. Definitions and examples of contamination are given in Table 1.
- Patients undergoing emergency (surgery on an unplanned admission) or elective (surgery on a planned admission) operations.
- Any operative indication, including trauma surgery.
- Patients able and willing to provide written informed consent (signature or a fingerprint).
- Adult and paediatric patients
NB: This criteria is country-specific. Each country decides the lower age limit for the trial. This is dependent on country-specific regulatory approvals. Age eligibility varies by country
- Patients with a documented or suspected allergy to iodine, shellfish, or chlorhexidine skin preparation solution.
- Patients unable to complete post-operative follow-up (i.e. will not be contactable after discharge).
Sponsor
The University of Birmingham is the Sponsor of the FALCON Trial in all collaborating countries.
International Coordinating Centre
The International Coordinating Centre FALCON trial office is at the University of Birmingham Clinical Trials Unit.
Each country will appoint a National Coordinating Investigator (NCI) and a National Coordinating Centre (NCC) – the Hub – who will take national responsibility for the study. The Hubs will be responsible for coordinating recruitment from a range of representative local hospitals – Spokes.
Central and National Trial Management Groups
The Central Trial Management Group (CTMG) includes those individuals responsible for the day-to-day management of the trial. This will include the trial CI, lead methodologists, patient representatives and FALCON central trial management staff.
Trial Steering Committee
The Trial Steering Committee provides overall supervision of the trial and ensures that the trial is being conducted in accordance with the principles of Good Clinical Practice and other relevant regulations.
Data Monitoring Committee
The Data Monitoring Committee will give advice on whether the accumulated data from the trial, together with the results from other relevant research, justifies the continuing recruitment of further participants.

Central Trial Management Group (University of Birmingham)
FALCON Trial Team
Birmingham Clinical Trials Unit, Public Health Building
University of Birmingham, Edgbaston, B15 2TT
Email: falcon@trials.bham.ac.uk
Tel: from UK 0121 414 4762, International +44121 414 4762